I often describe the dedication involved with a career in research as well as how scientists can spend their entire careers studying a very specific aspect of a disease process. I enjoyed reading this article about Dr. Kati Kariko, a Hungarian-born scientist, whose research laid the foundation for the future of the mRNA vaccines which today protect us against COVID-19.
Author: nicolemgatto
CDC Interim Guidance for Fully Vaccinated Adults
The CDC has released preliminary guidance for adults who have been fully vaccinated against COVID-19. The guidance outlines what activities fully vaccinated adults can safely do at this stage when still the majority of the population have yet to be vaccinated. By definition, “fully vaccinated” means 2 weeks since receiving the second dose of the Moderna or Pfizer vaccine OR the one-dose Johnson & Johnson vaccine. What do public health experts think about the guidance? In my case, while I’m fully vaccinated as of Thursday I am still wearing my mask and taking other precautions when in public!
why do COVID death rates differ by country?
Interesting article in the New Yorker COVID-19 death rates by country
Evidence for COVID-19 benefit from vitamin D?
An interesting question which will require additional research is whether vitamin D may play a role in COVID-19. Vitamin D is known to be essential to immune function. Some initial research suggests that vitamin D may reduce COVID-19 severity by suppressing the cytokine storm in COVID-19 patients. Vitamin D deficiency is more common among persons with naturally dark skin. The pigment (melanin) in dark skin doesn’t absorb as much UV radiation, which stimulates natural skin production of vitamin D. This may contribute to an explanation for why African-American and Latinos in the US are more likely to become infected with SARS-CoV2 and experience more severe COVID-19, including being more likely to die from the disease.
A recent study of 14,000 members of an Israeli HMO who were tested for SARS-CoV2 infection from February 1st to April 30th, 2020, and who had at least one previous blood test for plasma vitamin D levels found that low plasma vitamin D levels were associated with an increased likelihood of COVID-19 infection and of hospitalization due to COVID-19.
Undoubtedly more research will continue to shed light (excuse the pun) on this topic.
Is SARS-CoV2 transmissable via aerosols?
That is one of the (many) million dollar questions during this COVID-19 pandemic. Whatever the answer, public health recommendations to wear masks and keep distance from others are both necessary and precautionary as cases continue to rise in the United States. An excellent review of the science by Jayaweera et al. is found here: https://www.sciencedirect.com/science/article/pii/S0013935120307143?via%3Dihub. Conclusion: we need more research to understand the virus as well as to make evidence-based decisions around prevention.
Webinar: The Epidemiology of COVID-19 at 6 months: 10 things we know and 10 we don’t
Friday, June 19, 2020 at 11:00 AM
As we arrive at the 6-month mark from when the world was first introduced to SARS-CoV2 from its origins in Hubei province, China, scientists, medical doctors and public health professionals have been working at a frenzied pace to understand the new virus. This webinar will review what is currently known about the epidemiology COVID-19, the disease caused by the virus, and discuss what we still need to learn. The presentation will include an overview of core concepts in epidemiology which we will apply to our discussion.
To watch a recording of the webinar: https://tinyurl.com/ycwe4uqa
Racial/ethnic disparities in COVID-19
Preliminary data from California on COVID-19 cases and deaths through May 20, 2020 suggest racial/ethnic disparities in adults diagnosed and dying from the disease caused by the novel coronavirus, SARS-CoV2. While there were substantial amounts of missing data (30% of cases and 2% of deaths were missing information on race/ethnicity) and data are dependent on testing to identify cases, two patterns have emerged. First, adults of Latino and Native Hawaiian/Pacific Islander race/ethnicity are disproportionately more likely to be infected with SARS-CoV2 relative to the proportion of the California population that they make up. Adults of African-American/Black race/ethnicity made up a greater proportion of deaths from COVID-19 relative to their proportion of the California population. The demographic data do not tell us why these patterns may exist but some hypotheses have been put forth. Cases, which indicate infection with COVID-19, may be associated with socioeconomic factors, such as, employment in essential occupations, being less able to work from home or less able or compliant with social distancing. Deaths, which indicate more severe disease once infected, may be reflective of less access to health services, more prevalent comorbidities, or vitamin D deficiency (vitamin D is essential to immune function). More research is needed to examine these potential racial/ethnic disparities.
The earliest images of coronaviruses
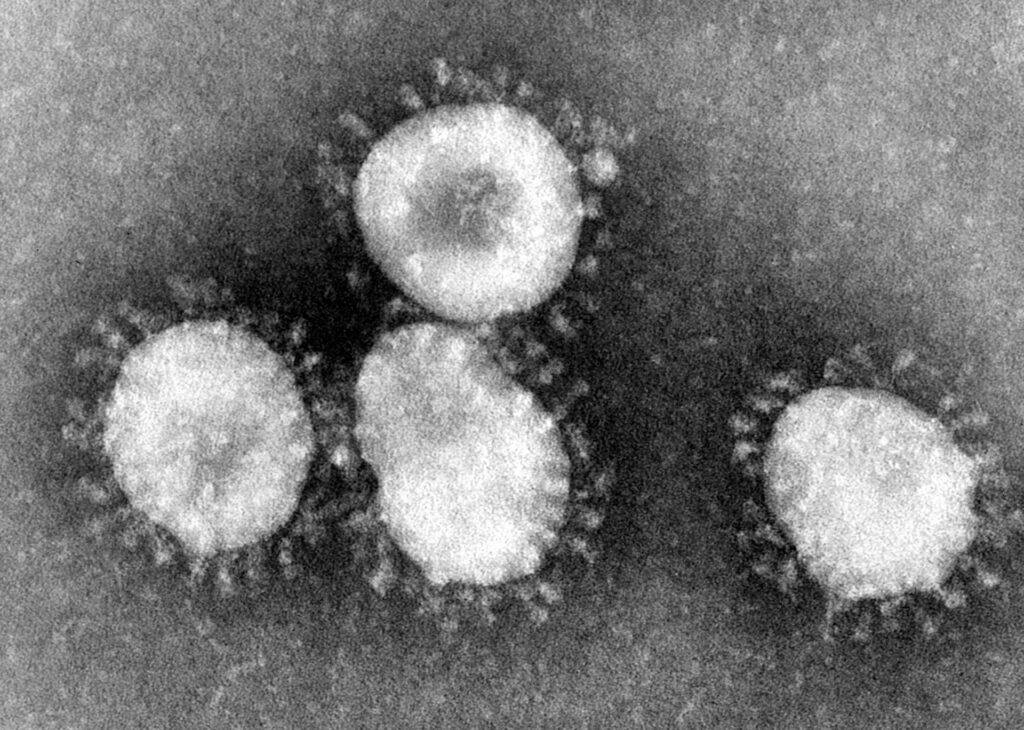
Ever wonder how scientists were first able to get a glimpse at coronaviruses? In 1964, a female virologist named June Almeida with an acumen for viral imaging using the electron microscope visualized coronaviruses for the first time. A recent National Geographic magazine article describes her microscopy techniques which allowed researchers at the time to discern one virus from another as well as to identify viruses that were previously unseen. And as it turns out, researchers today are still using her techniques to accurately identify viruses.
Pandemic EpiSpeak

Students who have taken one of my classes in epidemiology at CGU will probably remember me saying that learning epidemiology is, in many ways, comparable to learning a new language. Like many other fields, in epidemiology, we use specific words to indicate specific things. Hopefully my students are having fond memories right about now of the terminology we learned in class, for example, to describe disease occurrence in populations.
Our “EpiSpeak” also includes terms used in efforts control epidemics, as we are currently with the COVID-19 pandemic. I’ve heard some mixing of terms circulating such as referring to our stay-at-home order as “quarantining”.
Here is some clarity on three key terms: isolation, quarantine and physical distancing (also called social distancing) citing the World Health Organization.
“Isolation means separating people who are ill with symptoms of COVID-19 and may be infectious to prevent the spread of the disease.”
“Quarantine means restricting activities or separating people who are not ill themselves but may have been exposed to COVID-19.” By anticipating who might become sick, the goal is to prevent spread of the disease at the time when people just develop symptoms.
“Physical distancing means being physically apart. WHO recommends keeping at least 1-metre (3 feet) distance from others. This is a general measure that everyone should take even if they are well with no known exposure to COVID-19.” A goal of physical distancing is to slow the spread of disease by reducing the number of interactions we have with each other.
Be a steward of epi and apply these terms precisely! A benefit of this, I hope, is that we can reduce some of the confusion that is circulating and help to answer the question, “what can I do in the face of this pandemic”?
Inhale: Spring!

With all the scents of spring in the air, the least sensible thing I’ve done is to hesitate to breathe deeply the aromas fearing what else I’d take to my lungs!